

Breast Cancer
Breast cancer is the uncontrolled growth of abnormal cells that can develop in one of several areas of the breast, including the
- ducts that carry milk to the nipple
- small sacs that produce milk (lobules)
- non-glandular tissue.
Breast cancer is considered invasive when the cancer cells have penetrated the lining of the ducts or lobules. That means the cancer cells can be found in the surrounding tissues, such as fatty and connective tissues or the skin. Noninvasive breast cancer (in situ) occurs when cancer cells fill the ducts or lobules but haven’t spread into surrounding tissue.
Forms of invasive breast cancer
- Invasive ductal carcinoma – This type of breast cancer, which accounts for three-quarters of cases, develops in the milk ducts. It can break through the duct wall and invade the fatty tissue of the breast. It can then spread (metastasize) to other parts of the body through the bloodstream or lymphatic system.
- Invasive lobular carcinoma – This type of breast cancer accounts for about 15% of cases. It originates in the breast’s milk-producing lobules. It can spread to the breast’s fatty tissue and other places in the body.
- Medullary, mucinous, and tubular carcinomas – These slow-growing breast cancers account for about 8% of breast cancers.
- Paget’s disease – This is a rare form of breast cancer. It starts in the milk ducts of the nipple and can spread to the dark circle around the nipple (areola). Women who get Paget’s disease usually have a history of nipple crusting, scaling, itching, or inflammation.
- Inflammatory carcinoma – This is another rare form of breast cancer. It can seem like an infection, because there is usually no lump or tumor. The skin is red, warm, and looks pitted like an orange peel. Because it spreads quickly, inflammatory carcinoma is the most aggressive and difficult to treat of all breast cancers.
Noninvasive or Precancerous Conditions
As more women have regular mammograms, doctors are detecting many noninvasive or precancerous conditions before they become cancer. These conditions include:
- Ductal carcinoma in situ (DCIS) – This occurs when cancer cells fill the ducts but haven’t spread through the walls into fatty tissue. Nearly all women diagnosed at this early stage can be cured. Without treatment, about 20% of DCIS cases will lead to invasive breast cancer within 10 years.
- Lobular carcinoma in situ (LCIS) – This is less of a threat than DCIS. It develops in the breast’s milk-producing lobules. LCIS doesn’t require treatment, but it does increase a woman’s risk of developing cancer in other areas of both breasts.
Risk Factors
A woman’s risk of developing breast cancer increases with age; more than three out of four breast cancer cases occur in women over age 50. Other risk factors for breast cancer include:
- having close relatives, such as a mother, sister, or grandmother, who have had the disease
- being of Ashkenazi Jewish descent
- having had chest radiation for another cancer, such as Hodgkin disease, especially if the radiation was received before the age of 30.
- having already had the disease or certain other abnormalities of breast tissue
- increased exposure to the female hormone estrogen — by having a first menstrual period before age 13, entering menopause after age 51, or using estrogen replacement therapy for more than 5 years
- never having been pregnant, or having a first pregnancy after age 30
- being overweight, especially after menopause
- drinking alcohol (cancer risk doubles with three or more drinks per day)
- having a sedentary lifestyle with little regular exercise.
- having undergone a prior breast biopsy
Although breast cancer is about 100 times more common in women than in men, men can develop the disease.
Symptoms
- a lump or thickening in the breast or under the arm
- a clear or bloody discharge from the nipple
- crusting or scaling of the nipple
- a nipple that no longer sticks out (inverted)
- redness or swelling of the breast
- dimpling on the breast skin resembling the texture of an orange
- a change in the contours of the breast, such as one being higher than the other
- a sore or ulcer on the skin of the breast that does not heal.
- Ultrasound can confirm whether the lump is a solid tumor or a fluid-filled, noncancerous cyst. It can also be used to assess any abnormal areas found on a mammogram.
Cancer Grades
Although it is not routinely performed, MRI is used to assess abnormalities on a mammogram, get a more accurate estimate of a cancer’s size, and check for other cancers. MRI can also be used for screening in woman at high risk of breast cancer. Examples include:
- presence of a genetic mutation of the BRCA gene,
- a first degree relative of a BRCA carrier
- a strong family history of breast cancer
- prior radiation to the chest wall between the ages of 10 and 30.
- If the lump is solid, your doctor probably will recommend a breast biopsy. During a biopsy, a small amount of breast tissue is removed and analyzed in a laboratory. Sometimes, your doctor will recommend a biopsy without doing an ultrasound or MRI first.
A breast biopsy can be done in different ways. These include
- fine-needle aspiration, which uses a thin needle to withdraw bits of tissue from the tumor
- large core needle biopsy, which allows larger pieces of tissue to be removed
- stereotactic needle biopsy, a type of large core needle biopsy, which uses special imaging equipment to pinpoint the tissue to be removed
- surgical biopsy, which involves removing all or part of the breast lump.
- The type of biopsy your doctor chooses will depend on the location of the lump, its size, and other factors.
A specialist called a pathologist will examine the tissue under a microscope determine whether the tissue contains cancer cells. If it does, the pathologist can determine the type of breast cancer.
The pathologist will also assign a grade to the cancer. The grade indicates how closely the cancer cells resemble normal cells. A lower grade means that the cancer is slower-growing and less likely to spread; a higher grade means that the cancer is aggressive and likely to spread. The grade is one factor doctors consider when planning treatment. The pathologist may also determine how rapidly the cancer cells are dividing.
Depending on the type of biopsy and whether neighboring lymph nodes were removed, the biopsy report may include additional information. For example, the report may clarify how much the cancer has spread.
Another important step is to determine whether the cancer cells are “hormone-receptor positive” for estrogen and progesterone. Receptors allow specific substances, such as hormones, to latch on to the cell. Normal breast cells have both estrogen and progesterone receptors.
Cancer cells may have both receptors, one receptor, or no receptors. Women who have hormone-receptor positive cancers generally have a better prognosis. That’s because they are more likely to respond to hormone therapy.
The biopsy sample should also be tested for a growth-promoting protein called HER2. The HER2 gene tells the cell to make the HER2 protein. Cancers with multiple copies of the HER2 gene produce too much HER2. These cancers, called HER2-positive, tend to grow and spread quickly.
This kind of information helps to guide treatment decisions. For example, women with HER2-positive cancers are likely to benefit from drugs that target the HER2 protein.
You may need to have additional tests to determine whether the cancer has spread. These include:
- bone scans
- CT (computed tomography) scans
- PET scans. PET scans look for metabolically active tissue. They are most useful to look for cancer that may have spread to other parts of the body.
Expected Duration
Breast cancer will continue to grow and spread until it is treated.
Prevention
Although there are no guarantees, you can take steps to help prevent breast cancer:
- Maintain a healthy weight.
- Exercise regularly.
- Limit your use of alcohol. (Experts recommend no more than one drink per day for women and two drinks per day for men.) If you do drink, you may decrease your breast cancer risk by taking a folate supplement.
- Get regular mammograms. Experts differ on whether women at average risk for breast cancer should start screening at age 45 or age 50. They also differ on the frequency of mammography, either yearly or once every 2 years. Ask your doctor what makes sense for you.
- Women who believe they may be at high risk of hereditary breast cancer should consider talking to a genetic counselor. This may influence the type and frequency of breast cancer screening they need.
Diagnosis
Your doctor will ask whether you have any risk factors for breast cancer, especially whether the disease runs in your family. He or she will then examine your breasts, looking for any signs and symptoms of breast cancer. These include a lump or thickening in your breast, nipple inversion or discharge, swelling or changes in breast contour, redness or dimpling of breast skin, and enlarged lymph nodes under your arm.
If your doctor discovers a lump or your screening mammogram detects an area of abnormal breast tissue, your doctor recommends additional tests for breast cancer. If you haven’t yet had a mammogram, that may be the next step. But in other cases, the next step is an ultrasound or magnetic resonance imaging (MRI).
Some women inherit mutations in the so-call breast cancer genes—BRCA1 and BRCA2. These genetic mutations put them at very high risk of developing breast and ovarian cancer. These women require more frequent screening, often with MRI. Some women opt to have their breasts and ovaries removed. This is the best way to prevent breast and ovarian cancer.
Treatment
Treatment for breast cancer usually begins with a decision about the type of surgery. Factors taken into consideration include:
- The type of breast cancer that has been diagnosed
- The characteristics of the original biopsy material
- Patient preferences
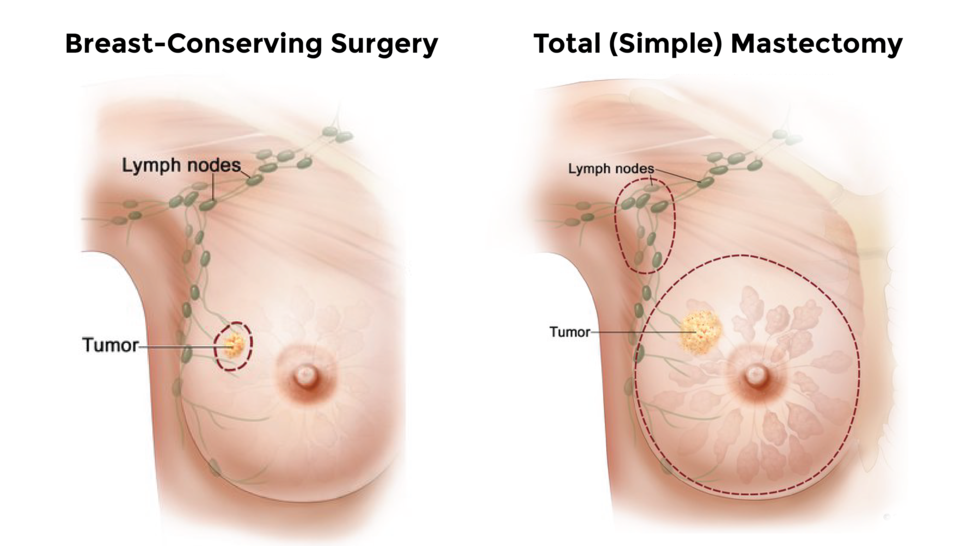
A mastectomy removes the entire breast, usually with removal of some of the lymph nodes located in the axilla or arm pit. A lumpectomy removes only the cancerous tumor and a small amount of healthy tissue around it.
The cancerous breast tissue removed during surgery may undergo further analysis. This can include looking for certain molecular and genetic characteristics that sometimes influence decisions regarding additional therapy. In addition, the results may provide information relevant to cancer risk in family members.
After surgery, your doctor may recommend radiation therapy, chemotherapy, hormone therapy, targeted therapy, or a combination of therapies. Additional therapies decrease the risk of cancer returning or spreading. Radiation therapy usually is recommended after a lumpectomy to destroy any cancer cells left behind and to prevent the cancer from returning. Without radiation therapy, the odds of the cancer returning increase by about 25%.
The need for chemotherapy depends on how much the cancer has spread and the molecular characteristics of the cancer. In some cases, chemotherapy is recommended before surgery to shrink a large tumor so that it can be removed more easily. Chemotherapy is usually necessary if cancer returns.
Hormone therapy usually is recommended if the cancer is estrogen-receptor positive. The drug most often used in these cases is tamoxifen. It locks estrogen out of breast cancer cells that are estrogen-receptor positive. (Estrogen can help cancer cells grow.) This may reduce the chances that the cancer will return by up to 30%.
Aromatase inhibitors are another form of hormone therapy. These drugs decrease the amount of estrogen in the body by blocking estrogen production in all other tissues except the ovaries. Aromatase inhibitors are most useful in menopausal women, because the ovaries stop making estrogen after menopause.
Drugs that target specific genetic changes to attack cancer cells are called targeted therapies. For example, if you breast cancer is HER2-positive, your doctor may offer you trastuzumab (Herceptin). This drug is a manmade version of an immune system protein. It attaches itself to the HER2 receptor, slowing the growth of cancer. It may also stimulate your immune system to mount a stronger attack.
Other drugs are being developed that help in the treatment of women who carry a genetic trait that exposes them to a type of breast or ovarian cancer that runs in families.
There is current controversy regarding the best treatment for DCIS – Ductal Carcinoma In Situ. Removal of the cancer by lumpectomy followed by radiation therapy has been the standard recommendation. However, for some women, complete removal of the area with a lumpectomy only may be sufficient. In cases where DCIS occurs in more than one location or if the tumor cells look especially worrisome on biopsy, the doctor may recommend mastectomy. Lymph nodes might also be removed as part of the mastectomy.
In most cases, LCIS – Lobular Carcinoma In Situ has a lower likelihood of progressing to invasive cancer, so little or no treatment is required. However, women with this condition are more likely to develop cancer in other areas of the same breast or other breast. So, they should have regular mammograms and breast exams. To decrease breast cancer risk, some women use hormone therapy, such as tamoxifen.
Based on your genetic markers, your doctor can choose the drugs that are most likely to attack your cancer. He or she may look to genetic markers to determine the chances that your breast cancer will spread to another site.
Call a Professional
Call your doctor immediately if you feel a lump or abnormal thickening in your breast. Call your doctor if you notice
- a new inverted nipple
- fluid dripping from one nipple
- swelling in a breast or a change in its contour
- redness or dimpling of breast skin.
Prognosis
Early diagnosis significantly improves the outlook for women with breast cancer. If the tumor is small and confined to the breast, more than 90% of women survive five years or longer. However, if the disease spreads throughout the body before diagnosis, that rate drops to less than 20%.
Cancer in one breast puts you at higher than average risk of developing cancer in the other breast. This is true even if you are still being treated with an estrogen blocker. Be sure to have regular checkups and mammograms.